Every cardiac arrest generates valuable data, but this data is useless unless it is systematically captured and analyzed. PACE implements a standardized data collection system that automatically documents:
CPR quality metrics:
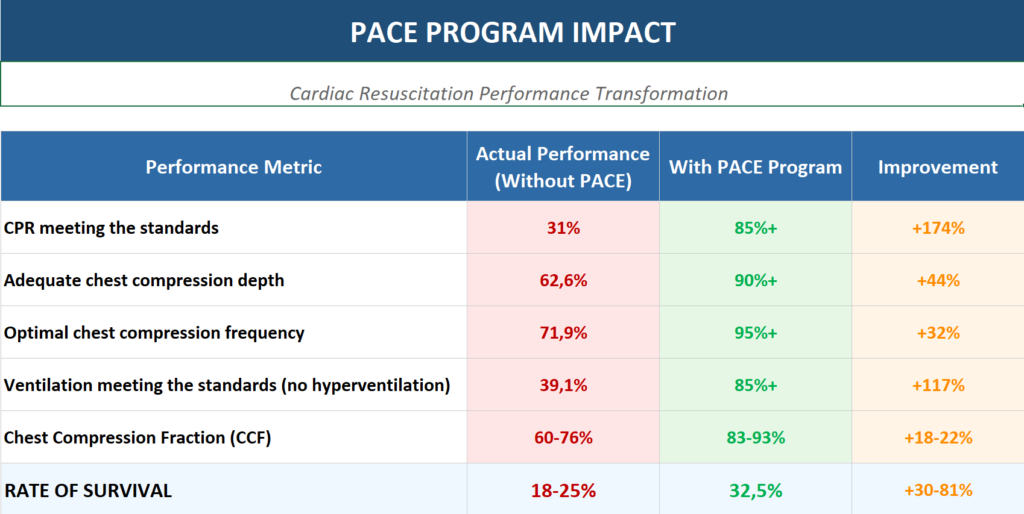
Chest compression fraction (CCF) – target >80%, ideally >90%
Average depth and percentage of compliant compressions (5–6 cm)
Average rate and compliance (100–120/min)
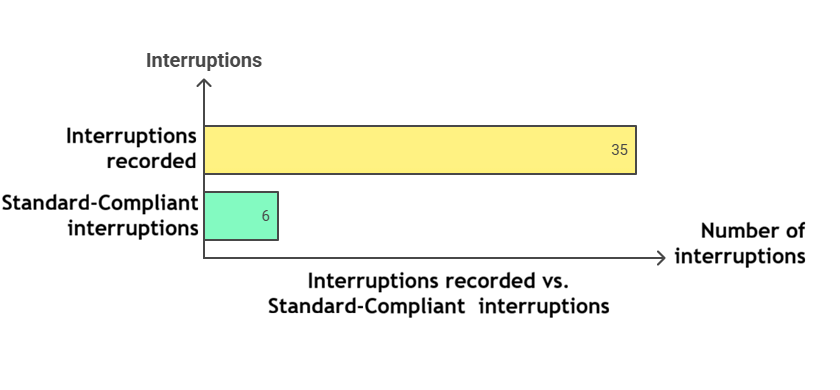
Number and duration of each interruption
Pre-shock and post-shock intervals
ETCO₂ values during resuscitation
Ventilation quality metrics:
Average respiratory rate (target: 10/minute)
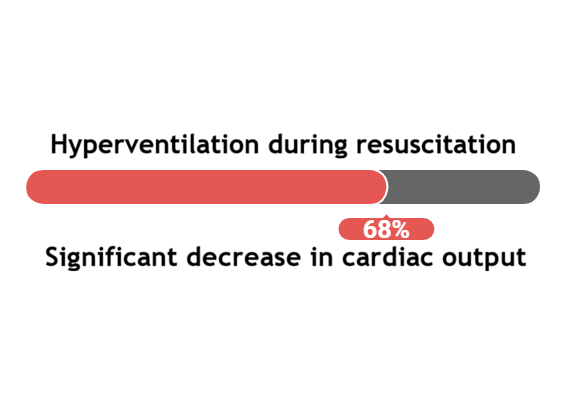
Percentage of time in hyperventilation (>10/minute)
Average tidal volume (target: 430–500 mL)
Percentage of ventilations with excessive volume
Process metrics:
Time to first defibrillation (target <2 minutes)
Time to first vasopressor (target <5 minutes)
Duration of intubation and associated interruptions
Duration of echocardiographic assessments
Time to installation of mechanical devices (LUCAS/AutoPulse)
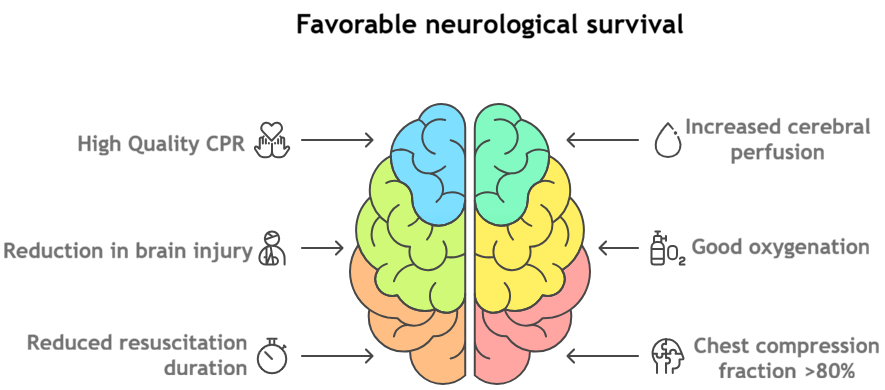
Clinical outcomes:
Return of Spontaneous Circulation (ROSC)
24-hour survival
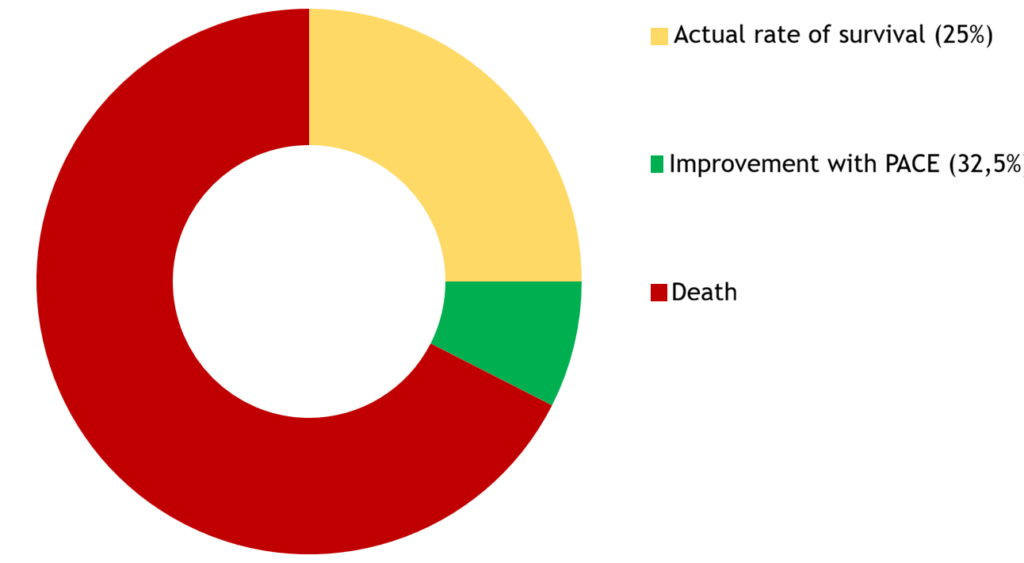
Survival at hospital discharge
Neurological status (CPC/mRS)
This data is extracted from defibrillators, compression and ventilation feedback devices, and medical records, then integrated into visual dashboards that enable a quick and clear analysis of your performance.